-
Author
Athreya Steiger -
PI
Maureen McCollough, MD, MPH
-
Co-Author
Ethan Forsgren, MD, MPH; Yesenia Perez, BA; Maureen McCollough, MD, MPH; Breena Taira, MD, MPH
-
Title
Patient Perspectives on Naltrexone Prescription from the ED for Alcohol Use Disorder
-
Program
STTP
-
Other Program (if not listed above)
-
Abstract
Title: Patient Perspectives on Naltrexone Prescription from the ED for Alcohol Use Disorder
Authors: Athreya Steiger, BS; Ethan Forsgren, MD, MPH; Yesenia Perez, BA; Maureen McCollough, MD, MPH; Breena Taira, MD, MPH
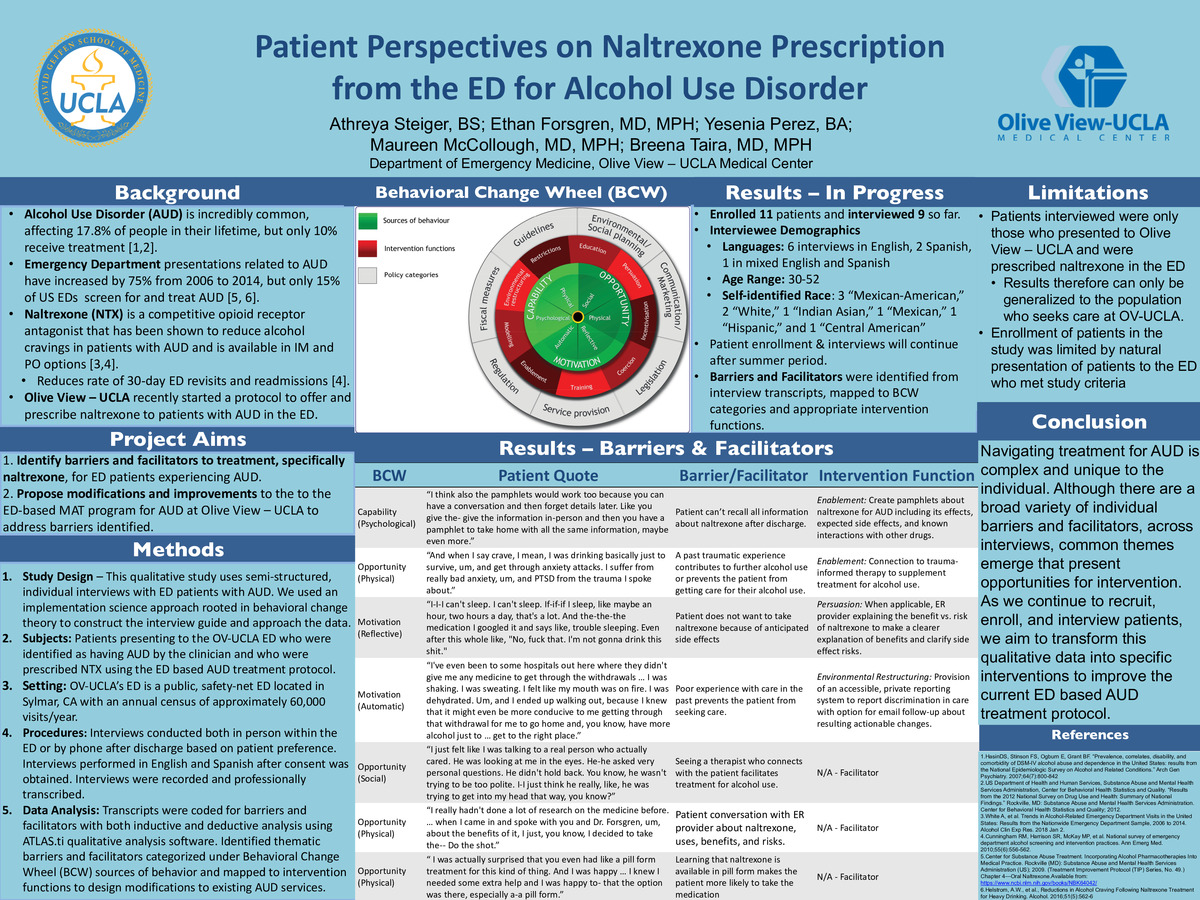
Background: Alcohol Use Disorder (AUD) is a frequent diagnosis in the Emergency Department. However, after the acute need is stabilized (withdrawal, vomiting, etc.), most ED patients with AUD are referred to primary care rather than starting treatment in the ED. For many of these patients, the ED is a missed opportunity for initiating medication assisted therapy for AUD. Last year, Olive View–UCLA implemented an ED based program to initiate naltrexone (NTX) for patients with AUD. NTX is the first-line treatment for AUD and reduces alcohol cravings.
Objective: Our study aims to identify barriers and facilitators to accepting and initiating AUD treatment, such as NTX, among patients who present to the Emergency Department. Data from this study will be used to improve the ED based AUD treatment protocol.
Methods:
Study Design: This is a qualitative study using semi-structured, individual interviews with ED patients with AUD. We used an implementation science approach rooted in behavioral change theory to construct the interview guide and approach the data.
Subjects: Patients presenting to the ED at OV-UCLA who were identified as having AUD by the clinician and who were prescribed NTX using the ED based AUD treatment protocol.
Setting: The OV-UCLA ED is a public, safety-net ED located in Sylmar, CA with an annual census of approximately 60,000 visits/year.
Procedures: Interviews were conducted both in person within the emergency department or over the phone after discharge based on patient preference. Interviews were performed in English and Spanish after written, informed consent was obtained. Interviews were recorded and professionally transcribed.
Data Analysis: Transcripts were then coded for barriers and facilitators through both inductive and deductive analysis using ATLAS.ti qualitative analysis software.
Identified thematic barriers and facilitators were categorized under Behavioral Change Wheel (BCW) sources of behavior and mapped to intervention functions to design modifications to existing AUD services.
Results: 11 patients were enrolled in the study, 9 of which are included in this data set. Interviewee ages ranged from 30-52. Six interviews were held in English, 2 in Spanish, and 1 in mixed English and Spanish.
Barriers identified include limited knowledge about NTX, fears of NTX side effects, and past experiences with discrimination in healthcare. Facilitators identified include ER provider advice to start NTX, seeing a therapist the patient connects with, and support from family. These barriers were then mapped to appropriate intervention functions as shown below.
BCW
Patient Quote
Barrier/Facilitator
Intervention Function
Capability
(Psychological)
“I think also the pamphlets would work too because you can have a conversation and then forget details later. Like you give the- give the information in-person and then you have a pamphlet to take home with all the same information, maybe even more.”
Patient can’t recall all information about naltrexone after discharge.
Enablement: Create pamphlets about naltrexone for AUD including its effects, expected side effects, and known interactions with other drugs.
Opportunity
(Physical)
“And when I say crave, I mean, I was drinking basically just to survive, um, and get through anxiety attacks. I suffer from really bad anxiety, um, and PTSD from the trauma I spoke about.”
A past traumatic experience contributes to further alcohol use or prevents the patient from getting care for their alcohol use.
Enablement: Connection to trauma-informed therapy to supplement treatment for alcohol use.
Motivation
(Reflective)
“I-I-I can't sleep. I can't sleep. If-if-if I sleep, like maybe an hour, two hours a day, that's a lot. And the-the-the medication I googled it and says like, trouble sleeping. Even after this whole like, "No, fuck that. I'm not gonna drink this shit."
Patient does not want to take naltrexone because of anticipated side effects
Persuasion: When applicable, ER provider explaining the benefit vs. risk of naltrexone to make a clearer explanation of benefits and clarify side effect risks.
Motivation
(Automatic)
“I've even been to some hospitals out here where they didn't give me any medicine to get through the withdrawals … I was shaking. I was sweating. I felt like my mouth was on fire. I was dehydrated. Um, and I ended up walking out, because I knew that it might even be more conducive to me getting through that withdrawal for me to go home and, you know, have more alcohol just to … get to the right place.”
Poor experience with care in the past prevents the patient from seeking care.
Environmental Restructuring:Provision of an accessible, private reporting system to report discrimination in care with option for email follow-up about resulting actionable changes.
Opportunity
(Social)
“I just felt like I was talking to a real person who actually cared. He was looking at me in the eyes. He-he asked very personal questions. He didn't hold back. You know, he wasn't trying to be too polite. I-I just think he really, like, he was trying to get into my head that way, you know?”
Seeing a therapist who connects with the patient facilitates treatment for alcohol use.
N/A - Facilitator
Opportunity
(Physical)
“I really hadn't done a lot of research on the medicine before. … when I came in and spoke with you and Dr. Forsgren, um, about the benefits of it, I just, you know, I decided to take the-- Do the shot.”
Patient conversation with ER provider about naltrexone, uses, benefits, and risks.
N/A - Facilitator
Opportunity
(Physical)
“I was actually surprised that you even had like a pill form treatment for this kind of thing. And I was happy … I knew I needed some extra help and I was happy to- that the option was there, especially a-a pill form.”
Learning that naltrexone is available in pill form makes the patient more likely to take the medication
N/A - Facilitator
Conclusions: Navigating treatment for AUD is complex and unique to the individual. Although there are a broad variety of individual barriers and facilitators, across interviews, common themes emerge that present opportunities for intervention. As we continue to recruit, enroll, and interview patients, we aim to transform this qualitative data into specific interventions to improve the current ED based AUD treatment protocol.
-
PDF
-
Zoom
https://uclahs.zoom.us/j/96251382738?pwd=UVArL2ZIQTFKZE5JQWJRenJRZFpHdz09
