-
Author
Keeley Ravellette -
PI
Tamara Horwich MD, MS
-
Co-Author
Alex Mirman MD
-
Title
Impact of Traditional vs. Intensive Cardiac Rehabilitation on Long-Term Cardiovascular Outcomes in Patients with Coronary Artery Disease
-
Program
STTP
-
Other Program (if not listed above)
-
Abstract
Impact of Traditional vs. Intensive Cardiac Rehabilitation on Long-Term Cardiovascular Outcomes in Patients with Coronary Artery Disease
Keeley Ravellette, Alex Mirman MD, Tamara Horwich MD, MS
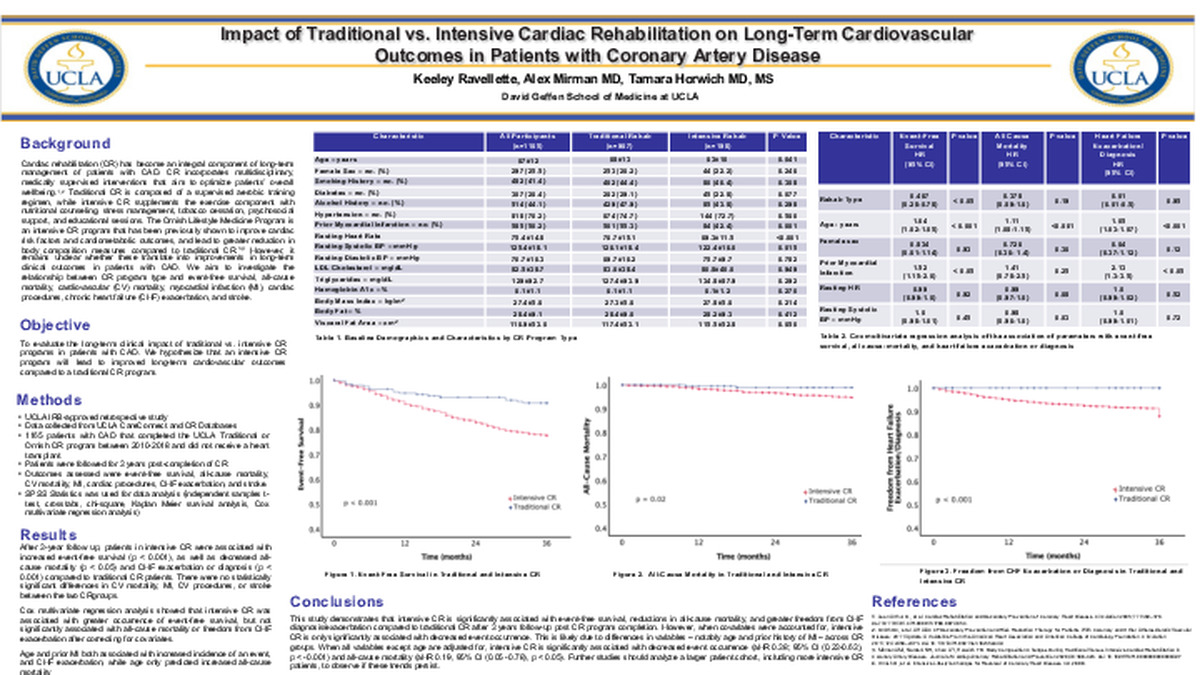
Background: Cardiac rehabilitation (CR) has become an integral component of long-term management of patients with CAD. Intensive CR has been shown to improve cardiac risk factors, cardiometabolic outcomes, and lead to improvements in body composition measures compared to traditional CR. However, it remains unclear whether these translate into improvements in long-term clinical outcomes in patients with CAD.
Aims: To evaluate the long-term clinical impact of traditional vs. intensive CR programs in patients with CAD. We hypothesize that an intensive CR program will lead to improved long-term cardiovascular outcomes compared to a traditional CR program.
Methods: Patients with CAD who completed either the UCLA Ornish Lifestyle Medicine Intensive CR program or a traditional CR program from 2010-2018 were followed for 3 years post-program completion. The main outcomes of interest were event-free survival, all-cause mortality, cardiovascular mortality, and incidence of MI, cardiovascular intervention (stent placement, CABG, valve repair, or heart transplant) and stroke. Data was collected using CareConnect and the UCLA CR Database.
Results: The study cohort consisted of 1165 patients with CAD (mean (SD) age, 67 (12) years; 25.5% (n=297) female), of which 967 participated in traditional CR (age, 68 (13); 26.2% (n= 253) female) and 198 in intensive CR (age, 63 (10); 22.2% (n=44) female). Intensive CR patients were younger, had fewer prior MIs, and lower resting heart rate (p < 0.05, respectively). In a follow-up period of 3 years, patients who participated in intensive CR were associated with increased event-free survival (p < 0.001), as well as decreased all-cause mortality (p < 0.05) and CHF exacerbation or diagnosis (p <0.001) compared to traditional CR patients. There were no statistically significant differences between CV mortality, incidence of MI, CV procedures, or stroke. Cox multivariate regression analysis showed that intensive CR was associated with greater occurrence of event-free survival, but not significantly associated with all-cause mortality or freedom from CHF exacerbation after correcting for covariates. Age and prior MI both predicted increased incidence of an event, as well as increased CHF exacerbation, while age only predicted increased all-cause mortality.
Conclusion: This study demonstrates that intensive CR is significantly associated with event-free survival, reductions in all-cause mortality, and greater freedom from CHF diagnosis or exacerbation compared to traditional CR after 3 years follow-up post CR program completion. However, when covariates were accounted for, intensive CR is only significantly associated with decreased event occurrence. Further studies should analyze a larger patient cohort, including more intensive CR patients, to observe if these trends persist.
-
PDF
-
Zoom
https://uclahs.zoom.us/j/98169279932?pwd=cklJTFcydCtQYlpCS0hBRE5yN0k5Zz09
