-
Author
Dustin Dillon -
PI
Mark Girgis, MD
-
Co-Author
Michael Mederos, MD; Joon Park, MD
-
Title
Enhanced Recovery Protocol Improves Hospital Length of Stay After Robot Assisted Pancreaticoduodenectomy
-
Program
STTP
-
Other Program (if not listed above)
-
Abstract
Background
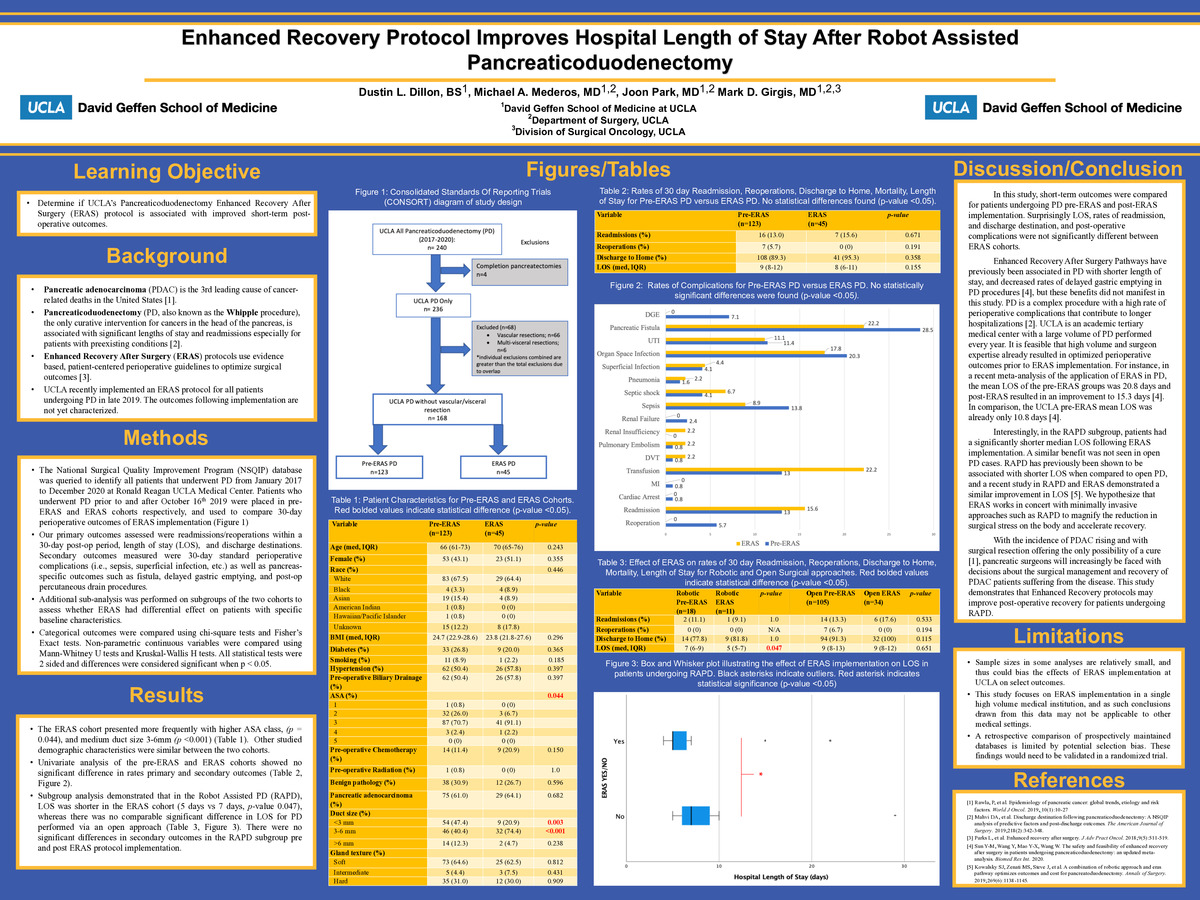
Pancreatic cancer is the 3rd leading cause of cancer-related deaths in the United States. Surgical resection offers the only possibility of a cure, with pancreaticoduodenectomy (PD, aka the Whipple procedure) being the most common operation. However, PD is a complex operation associated with significant morbidity. Enhanced Recovery After Surgery (ERAS) pathways utilize patient-centered and evidence-based protocols aimed at optimizing patients for surgery and facilitating post-operative recovery. These pathways have been shown to reduce length of stay within a variety of operations, including PD. UCLA recently implemented an ERAS protocol for all patients undergoing PD in late 2019. The purpose of this study was to characterize the effect of the UCLA PD ERAS pathway on short-term postoperative outcomes.
Methods
The National Surgical Quality Improvement Program (NSQIP) database was queried to identify all patients that underwent PD from January 2017 to December 2020 at Ronald Reagan UCLA Medical Center. Patients who underwent PD prior to and after October 16th, 2019 were placed in pre-ERAS and ERAS cohorts respectively and used to compare 30-day perioperative outcomes of ERAS implementation. Completion pancreatectomies, vascular resections, and multi-visceral resections were excluded.
Results
Median length of stay, readmission within 30 days, and reoperation within 30 days, and discharge to home were similar for ERAS PD versus pre-ERAS PD.
Secondary outcomes were also similar regarding rates of pancreatic fistula, delayed gastric emptying, renal insufficiency, renal failure, pneumonia, pulmonary embolism (PE), urinary tract infection (UTI), superficial infection, deep incisional infection, organ space infection, cerebrovascular attack (CVA), cardiac arrest, myocardial infarction (MI), bleeding/transfusions, deep vein thrombosis (DVT), sepsis, septic shock.
Subgroup analysis demonstrated that in patients undergoing Robot Assisted PD (RAPD), median length of stay was decreased (7 days vs 5 days). No such decrease was seen when analyzing the effect of ERAS in open PD cases. Rates of readmission, reoperation, discharge to home, and postoperative complications were similar between pre-ERAS and ERAS RAPD.
Conclusions
ERAS protocol implementation at UCLA was not associated with significant differences in perioperative outcomes, possibly due to the high quality of care at UCLA prior to ERAS implementation. However, ERAS implementation in RAPD cases decreased length of stay in the hospital demonstrating that ERAS protocols potentially magnify the benefits of minimally invasive surgical platforms.
-
PDF
-
Zoom
https://uclahs.zoom.us/j/93049175570?pwd=cm8zY2hyZDVqUkJiNkJLUkxTOVpWUT09
