-
Author
Samantha Garcia -
PI
Hei-Wah Wong, MD
-
Co-Author
Natalia Sejbuk, MPH; Manisha Ati, FNP-C; Tinh Vuong, DO
-
Title
Perceived Barriers and Benefits Toward Breast Cancer Screening Among Saban Community Clinic Patients
-
Program
Other
-
Other Program (if not listed above)
Jim Slotnick Fellowship in Medicine
-
Abstract
BACKGROUND:
Breast cancer is the most common cancer in the developed world and it is the second leading cause of cancer mortality among women [1]. In 2018, 254,744 new cases of breast cancer and 42,465 breast cancer related deaths were reported in the United States [2]. The prevalence of breast cancer is highest in white and non-hispanic black women [2]. The US Preventive Services Task Force’s current breast cancer screening guidelines suggest that women ages 50 to 54 years get screened with mammography annually [3]. For women ages 55 years and older, screening with mammography is recommended once every 1-2 years until 75 years of age [3]. Adherence to screening is imperative as it can lead to early diagnosis of breast cancer and reduce the risk of mortality by 26% for every 1,000 women screened [2,4]. Encouraging breast cancer screening among racial and ethnic minorities is imperative as breast cancer disparities exist among these groups. For instance, Hispanic women are less likely than white women to engage in routine mammography screening [5]. As a result, breast cancer is typically diagnosed at more advanced stages and there is a higher mortality rate in Hispanic women despite the low prevalence of breast cancer among this population [6]. In black women, breast cancer occurence is at a younger age, has less favorable clinical outcomes, and is associated with more aggressive tumor phenotypes [7]. Furthermore, screening for breast cancer is cost effective, since breast cancer represents 13% of all cancer treatment costs in the United States, the highest treatment cost of any cancer [2].
Saban Community Clinic (SCC) is a five site federally qualified health center (FQHC) that serves under-resourced and low-income populations in Los Angeles. Given that the patient population at SCC is 55% Hispanic, a demographic that faces poorer breast cancer outcomes, and 22% Caucasian, the demographic that has the highest prevalence of breast cancer, screening for breast cancer among the female patient population is crucial. Given the size of the Los Angeles region, transportation can be a barrier to access healthcare, especially for those who rely on public transportation or have limited access to a car. Many female patients were sent to Beverly Tower Women’s Health Center in Beverly Hills for their mammography services. Since these patients were sent offsite to a location that is far from many of SCC’s sites, this may affect the number of completed mammograms. In order to address some of these barriers to care, SCC partnered with ProLife, a company that provides mobile mammogram services. Presently, SCC hosts mobile mammogram clinics every other month at its Melrose clinic site. Patients are referred by their healthcare provider and a SCC outreach worker schedules appointments 1-week in advance. Patients receive a reminder call from a Patient Care Coordinator 1-2 days in advance to confirm their appointment.
While the mobile mammogram services have been successful overall, there continue to be patients who do not schedule an appointment once referred for a mammogram screening or do not attend a scheduled appointment. The present study explores the perceived barriers toward breast cancer screening among patients who have missed their annual mammogram appointment and explores their perceptions toward mammograms.
STUDY QUESTIONS:
-
What barriers toward breast cancer screening exist for patients who did not schedule or attend their mammogram appointment?
-
What perceptions do patients who did not schedule or attend their mammogram appointment have in regard toward the benefits of breast cancer screening?
-
What can Saban Community Clinicdo to address barriers patients face in attending mammogram appointments?
METHODS:
A 24-item survey was developed to assess perceived barriers and benefits toward breast cancer screening. 20 items on the survey were developed utilizing validated questions based on the Health Belief Model [8]. In past studies, these items were shown to measure benefits and barriers related to mammography behavior and to be reliable among diverse populations such as low-income, Hispanic, and African American women [6,8,9]. Patients were asked to respond to these 20 items on a 5-point Likert scale from strongly disagree to strongly agree. The survey items addressing perceived barriers were separated into 4 categories: psychological, knowledge, logistical, and immigration status barriers. 4 survey items were open-ended questions centered on patients’ experience with scheduling mammograms at SCC, interest in rescheduling or scheduling a mammogram appointment, reasons for not attending a scheduled appointment, and experience knowing someone diagnosed with breast cancer. Electronic medical records were used to obtain data on patients who had mammogram referrals ordered from November 2020-May 2021 but did not schedule their mammogram appointment or did not attend their scheduled appointment. Patients were contacted by phone and the survey was administered in a structured interview format.
RESULTS
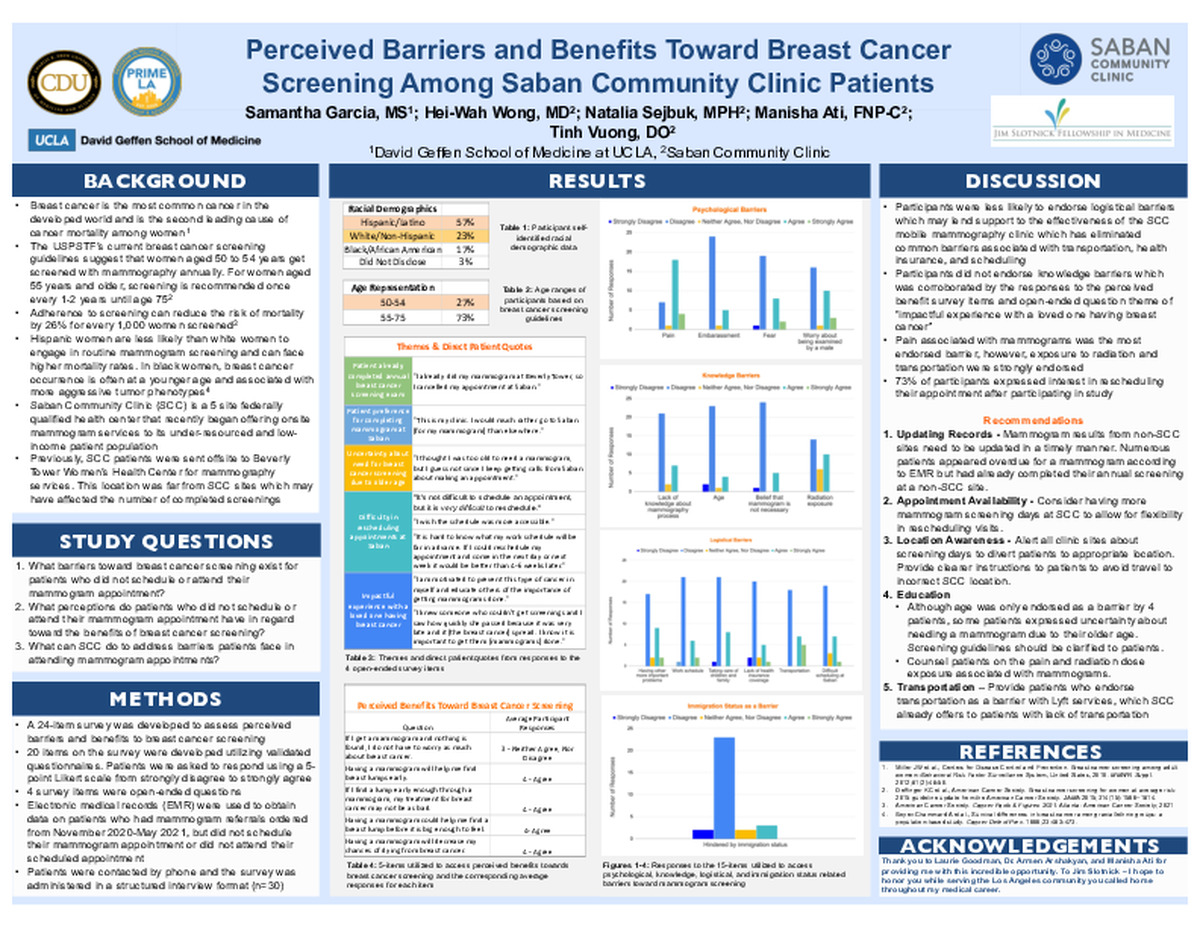
A total of 30 female patients participated. 57% (17 participants) identified as Hispanic/Latino, 23% identified as White/Non-Hispanic (7 participants), 17% identified as Black/African American (5 participants), and one participant did not disclose their racial demographic information. 27% of participants were between the ages of 50-54 and 74% were between the ages of 55-75. The average age of participants was 58 years old.
The average participant response for each barrier type was as follows:
-
Psychological barriers: 3- neither agree, nor disagree
-
Knowledge barriers: 2- disagree
-
Logistical barriers: 3- neither agree, nor disagree
-
Immigration status barriers: 2 - disagree
The average participant response for perceived benefits toward breast cancer screening was “4- agree” with the exception of the item “If I get a mammogram and nothing is found, I do not have to worry about breast cancer” which had an average response score of “3- neither agree, nor disagree.”
Direct quotations from patient responses to open-ended questions revealed 5 themes:
1. Patient already completed their annual breast cancer screening exam at an offsite location
2. Patient preference for completing mammograms at Saban
3. Uncertainty about the need for breast cancer screening due to older age
4. Difficulty in rescheduling mammogram appointments at SCC
5. Impactful experience with a loved one having breast cancer
Following completion of the survey, 22 patients (73% of participants) expressed interest in rescheduling their mammogram appointment.
DISCUSSION
From all perceived barrier survey items, pain associated with mammograms was the most endorsed barrier. When assessing participant responses toward logistical barriers, it was noted that participants were less likely to endorse these types of barriers. This may lend support to the effectiveness of the SCC mammography program, which has eliminated common barriers associated with transportation, health insurance, and scheduling. However, while 18 participants disagreed that lack of transportation was a barrier, 12 participants viewed it as a barrier.
Participants did not endorse most knowledge barriers which was corroborated by the responses to the perceived benefit survey items. In addition, representative quotes from the open-ended question theme “impactful experience with a loved one having breast cancer” revealed that many patients are aware of the importance of breast cancer screening and early detection. For instance, one patient shared "I knew someone who couldn't get screenings and I saw how quickly she passed because it was very late and it [the breast cancer] spread. I know it is important to get them [mammograms] done." However, it should be noted that radiation exposure was a knowledge related barrier endorsed by 10 participants.
Recommendations
-
Updating Records - Mammogram results from non-SCC sites need to be updated in a timely manner. Numerous patients appeared overdue for a mammogram according to EMR but upon calling them, they clarified that they had already completed their annual screening at a non-SCC site.
-
Appointment Availability - Consider having more mammogram screening days at SCC to allow for flexibility in rescheduling visits.
-
Location Awareness - Alert all clinic sites about screening days to divert patients to appropriate location (Melrose clinic site). Provide clearer instructions to patients to avoid travel to incorrect SCC locations.
-
Education - Although age was only endorsed as a barrier by 4 patients, some patients expressed uncertainty about needing a mammogram due to their older age. Screening guidelines should be clarified to patients. In addition, patients should be counselled on pain and radiation dose exposure associated with mammograms and address their concerns upon referral to SCC mammogram clinic.
-
Transportation - Provide patients who endorse transportation as a barrier with Lyft services, which SCC already offers to patients with lack of transportation.
REFERENCES:
-
Miller JW, King JB, Joseph DA, Richardson LC; Centers for Disease Control and Prevention (CDC). Breast cancer screening among adult women--Behavioral Risk Factor Surveillance System, United States, 2010. MMWR Suppl. 2012;61(2):46-50.
-
U.S. Cancer Statistics Working Group. U.S. Cancer Statistics Data Visualizations Tool, based on 2020 submission data (1999-2018): U.S. Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute; www.cdc.gov/cancer/dataviz, released in June 2021.
-
Oeffinger KC, Fontham ET, Etzioni R, Herzig A, Michaelson JS, Shih YC, Walter LC, Church TR, Flowers CR, LaMonte SJ, Wolf AM, DeSantis C, Lortet-Tieulent J, Andrews K, Manassaram-Baptiste D, Saslow D, Smith RA, Brawley OW, Wender R; American Cancer Society. Breast cancer screening for women at average risk: 2015 guideline update from the American Cancer Society. JAMA 2015;314(15):1599–1614.
-
American Cancer Society. Cancer Facts & Figures 2021. Atlanta: American Cancer Society; 2021
-
Boyer-Chammard A, Taylor TH, Anton-Cuver H. Survival differences in breast cancer among racial/ethnic groups: a population-based study. Cancer Detect Prev. 1999;23:463-473.
-
Medina-Shepherd R, Kleier JA. Spanish translation and adaptation of Victoria Champion's Health Belief Model Scales for breast cancer screening--mammography. Cancer Nurs. 2010;33(2):93-101. doi:10.1097/NCC.0b013e3181c75d7b
-
Wambui G. Gathirua-Mwangi, PhD(c), MPH, Patrick O. Monahan, PhD, Timothy Stump, MA, Susan M. Rawl, PhD, Celette Sugg Skinner, PhD, Victoria L. Champion, PhD, RN, FAAN, Mammography Adherence in African-American Women: Results of a Randomized Controlled Trial, Annals of Behavioral Medicine, Volume 50, Issue 1, February 2016, Pages 70–78, https://doi.org/10.1007/s12160-015-9733-0
-
Champion VL. Revised susceptibility, benefits, and barriers scale for mammography screening. Res Nurs Health. 1999;22(4):341-348. doi:10.1002/(sici)1098-240x(199908)22:4<341::aid-nur8>3.0.co;2-p
-
Champion VL, Monahan PO, Springston JK, et al. Measuring mammography and breast cancer beliefs in African American women. J Health Psychol. 2008;13(6):827-837. doi:10.1177/1359105308093867
-
-
PDF
-
Zoom
https://uclahs.zoom.us/j/91432203840?pwd=aXIzd1FJVlA5VnRVWFlNNzRHeHM3dz09
