-
Author
Joseph Ebriani -
PI
Berkeley Limketkai, MD, PhD
-
Co-Author
Joseph Ebriani, MS1, Vivy Casumano, MD, Patrick Holman, MD, Preeti Prakash, MD, and Berkeley Limketkai, MD, PhD
-
Title
Anti-TNF Failures: A Retrospective Cohort Study For Patients With Moderate-to-Severe Inflammatory Bowel Disease (IBD) seen at UCLA
-
Program
Internal Medicine Chief's Fellowship
-
Other Program (if not listed above)
-
Abstract
Background:
Biologic therapies are powerful and effective immunosuppressants for the induction and maintenance of remission in patients with moderate-to-severe inflammatory bowel disease (IBD). However, among patients who initiate a biologic agent, approximately 40-50% of them may not achieve clinical remission even after a year of treatment.1,2 While waiting to determine whether the patient might or might not eventually respond to therapy, there is a risk of delaying the switch to a potentially more effective biologic agent, deferring the need for surgical intervention, and unnecessarily prolonging patient suffering. However, there are currently insufficient data to reasonably predict which patients will ultimately respond to initial biologic therapy.3 The goals of the study are to characterize patterns of clinical response to first-time biologic therapy in patients with IBD and to identify clinical factors that predict early response, late response, and non-response to biologic therapies . We hypothesize that patients with higher inflammatory marker scores will exhibit a decreased response to certain anti-TNF therapies.
Methods:
A retrospective cohort study was conducted for patients with moderate-to-severe Crohn’s disease (CD) and ulcerative colitis (UC) seen at the UCLA Center for Inflammatory Bowel Diseases who initiatedfirst-line biologic therapy at UCLA. Exclusion criteria included use of biologics prior to starting care at UCLA and duration of follow-up at UCLA less than 6 months. Data of interest included: colonoscopy and pathology reports, prescribed biologic, Harvey Bradshaw Index (HBI) scores, Simple Clinical Colitis Activity Index (SCCAI) scores, C-Reactive Protein levels, fecal calprotectin, corticosteroid rounds, hospitalizations, extra-intestinal manifestations (EIMs) of IBD, family history of IBD, BMI, age, sex, ethnicity, and insurance status.
Data was abstracted from the electronic medical records and stored in REDCap, a Health Insurance Portability and Accountability Act (HIPAA)-secure database server hosted by the UCLA Clinical and Translational Science Institute (CTSI).
The study population was then subdivided into 3 groups based on response time: early-response, late-response, and non-response. Response time was measured as the time from initiation of anti-TNF therapy to 4 primary measures: 1) a colonoscopy score graded as mild or quiescent, 2) a fecal calprotectin score < 250 , 3) a CRP score <1.0, or 4) For CD patients, an HBI score ≤ 4, and for UC patients, an SCCAI score ≤ 2. If there was concordance between all 4 measures above, then the earliest date indicating remission was used to categorize the patient into a response group. Otherwise, the colonoscopy score was used as the gold standard to indicate whether the patient had achieved remission. As such, patients with a response time of less than 4 months were classified as early responders, while patients with a response time between 4 to 12 months were classified as late responders. Patients who took longer than 12 months to achieve remission or failed to reach at least one of the four markers were classified as non-responders. Descriptive analyses was then used to estimate the proportions and timing of response after initiation of anti-TNF therapy. Multivariable logistic regression was also used to identify variables that were associated with early-response, late-response, and non-response.
Results:
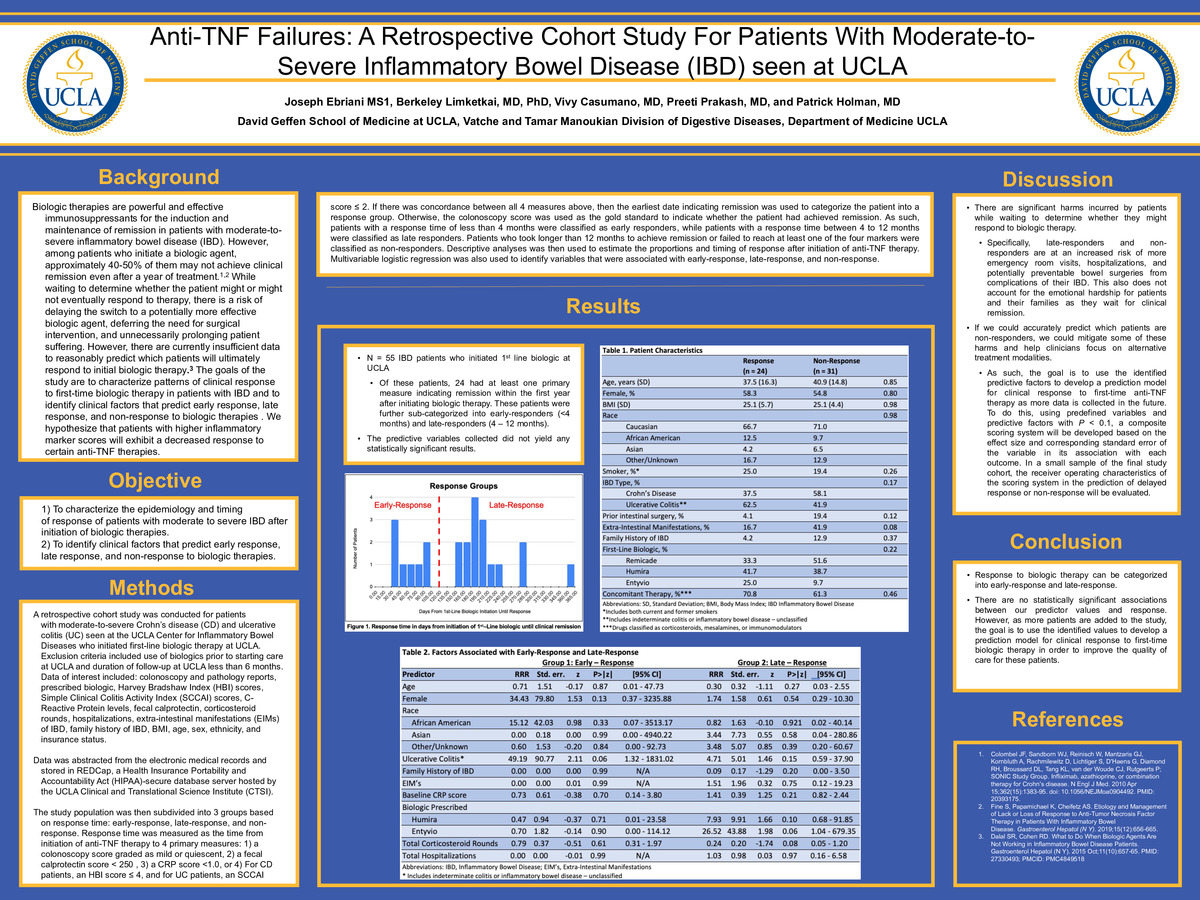
This study included 55 IBD patients who initiated 1st line biologic at UCLA. Of these patients, 24 had at least one primarymeasure indicating remission within the first year after initiating biologic therapy. These patients were further sub-categorized into early-responders (<4 months) and late-responders (4 – 12 months). The predictive variables collected did not yield any statistically significant results.
Discussion:
There are significant harms incurred by patients while waiting to determine whether they might respond to biologic therapy. Specifically, late-responders and non-responders are at an increased risk of more emergency room visits, hospitalizations, and potentially preventable bowel surgeries from complications of their IBD. This also does not account for the emotional hardship for patients and their families as they wait for clinical remission. Further, if we could accurately predict which patients are non-responders, we could mitigate some of these harms and help clinicians focus on alternative treatment modalities. As such, the goal is to use the identified predictive factors to develop a prediction model for clinical response to first-time anti-TNF therapy as more data is collected in the future. To do this, using predefined variables and predictive factors with P < 0.1, a composite scoring system will be developed based on the effect size and corresponding standard error of the variable in its association with each outcome. In a small sample of the final study cohort, the receiver operating characteristics of the scoring system in the prediction of delayed response or non-response will be evaluated.
Conclusion:
Response to biologic therapy can be categorized into early-response and late-response. Currently, there are no statistically significant associations between our predictor values and response. However, as more patients are added to the study, the goal is to use the identified values to develop a prediction model for clinical response to first-time biologic therapy in order to improve the quality of care for these patients.
-
PDF
-
Zoom
https://uclahs.zoom.us/j/3197231221?pwd=RjNlYnhNdTlPc2ZieWgxa3Z5b3Ezdz09
